 full-size
full-size full-size full-size full-size
full-size full-size full-sizeSo if we don’t control it, it will cause severe first order impacts: death and disease. The second and third order impacts we’re already seeing: education, economy, relationships of all kinds…
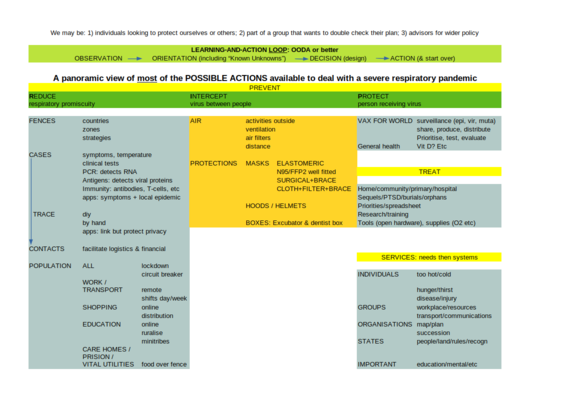
What if we at least regain control of what we do? Start by looking at this simplistic framework where all the “things we can do” are collected. Get to know our tools. Improve them, facilitate them, use them, combine them. Assist one another in overcoming this situation.
Details follow.
This virus goes from person A to person B. We want to stop that from happening. So we can only: 1. not have persons A and B in the same space, or 2. have them in the same space but have something in between that will catch the virus on its way from person A to person B, or 3. protect person B so that if the virus gets to person B it will have no effect.
Here, we call the first strategy REDUCE: we reduce the number of risky respiratory contacts. Ideally, we only reduce the contacts between infected A and non-infected B. But if there’s uncertainty (is A infected? is B immune?) then we need to use the second which is called INTERCEPT. And all of this would eventually stop if everyone is immune (PROTECT’ed, which is the third strategy).
The widest ranging one happens at BORDERS. It may be between countries or between regions inside a country - let’s call them “zones”. We want to stop the virus, or variants of the virus, from entering a new zone. We may do that by not allowing people in at all, or by allowing them in with tests and quarentine. We’ll talk about tests and quarentine later.
The narrowest, most precise one, is about ISOLATING CASES. Someone who has the virus stays in their own room until they are no longer contagious. This needs testing and assistance.
…